Medical Response Training and Equipment for Protective Services
As part of the big picture when providing protective services, the security, safety and reputation protection of the client are our main objectives. In this regard, the ability to provide medical response is a vital aspect as we will certainly be the ‘first responders’ at the point of wounding. Although this means we have already failed out main objective, ‘damage control’ and increasing the chances of survivability going forward are still your responsibility. In this article we’ll discuss appropriate training priorities, goals and equipment selection for providing point-of-wounding care in a realistic protective services scenario
Protective Medical Training Course
Perhaps the most critical aspect of medical response is factor of time – the faster aid is provided, the faster advanced medical response is initiated and the faster the patient is evacuated to urgent/traumatic care facilities the higher the chances of survivability. Specifically to massive hemorrhaging, your response must be initiated prior to irreversible blood loss occurs and this takes merely less than a minute, as little as 45 seconds.
–
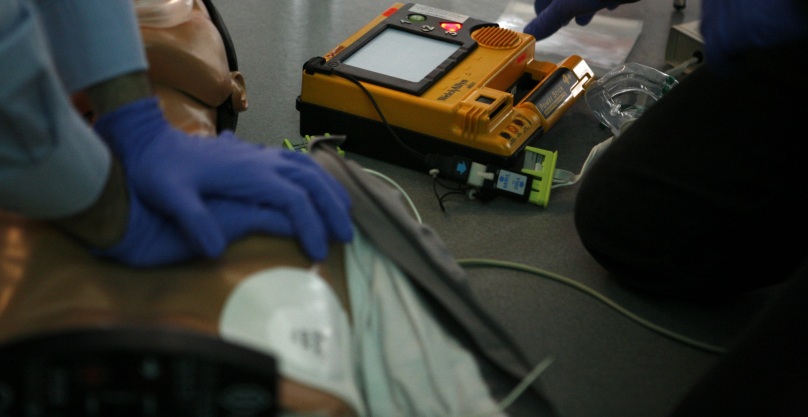
The Need

As you can see in the image above where Ambassador Lippert was slashed on the arm and face, there was no immediate medical kit available and only expedient methods were utilized. The patient survived, however the care would have been substantially more appropriate if any lf the first responders had an on-body medical kit. The simple fact of the matter is that protected individuals are under threat of intentional injuries and we are all under threat of unintentional injuries. With that being said, a minimal amount of training and preparedness goes a long way in medical response and there is no excuse not to be trained and certified at the basic level. Both intentional attacks and unintentional injuries can result in the need for first aid up to traumatic injuries, all of which you should be trained AND prepared to respond to.
–
Training Goals
As always, training should either provide knowledge or certify for a task. For medical training, seek both as the knowledge is critical and protecting yourself as a first responder is also important.The minimum training and certification requirement is Adult and Pediatric CPR, First Aid and AED training from the American Red Cross, American Heart Association or similar. With that being said, the minimum in this case is not a bad thing as you must understand that advanced medical training requires advanced equipment in which it will not be practical to have in 99.9% of cases. With this understanding, seem practical training for the most likely occurrences based on your task, threat and environment in relation to what equipment you can feasibly have available. For most applications, the most common traumatic injuries that result in preventable death can be categorized into exsanguination – massive hemorrhage from an extremity. This can be mitigated by a tourniquet, pressure bandage and/or hemostatic dressing. See the IPAK contents below for more info.
“In our line of work, a fair amount of medical training is important. If you work in a high threat environment TCCC or even Paramedic training would be in your best interest. If you work in a domestic setting with a client that is known to have their share of controversy, EMT training may still be an avenue you want to consider.
However, at a bare minimum you should be proficient with CPR, First aid and AED. As a professional protector, it is your job to know your client and by knowing your client, you should know ALL of their medical needs. But just because your client has not had any threats against them, there is no reason not to be prepared. Just having something as small as as the IPAK can save your client or even yourself in a unexpected situation. The ability to control bleeding more times than not will save the life of your principal or yourself before your gun will.
It is important to chose a medical training provider that has a practical application for what it is that you’re doing. As a state certified firefighter paramedic, I completely endorse the Lasorsa and Associates Protective Medical Training Course.” – Craig Butler, Darkmoon Protection, Inc.
–
Equipment Selection
Every protector should strongly consider an on-body medical kit designed for the most time sensitive life threatening situations, and this is exactly why we have designed the Individual Protective Agent’s Kit – IPAK. In addition to that, a more substantial kit would ideally be ‘immediately available’ or close by in the vehicle or in a bag carried by a team member.
–

Above: The Adventure Medical Kits ‘Comprehensive Kit’ with add-on trauma items, and an IPAK
–

Above: The contents of the Adventure Medical Kit with add-on trauma kit and the IPAK
–
In Response
“The following information is based on my twenty years as a NJ Certified EMT and fifteen years as an American Red Cross Emergency Medical Response Instructor. Additionally, this information is geared towards protection providers with a minimal to no experience or training in responding to medical emergencies in CONUS. Obviously should the need arise you should provide treatment to your level of certification and training.
–
–
The first thing any person needs to do when addressing a medical emergency is to stay calm and access the situation. Having some level of baseline knowledge regarding our principal’s medical history and conditions is always helpful. As that is not always the case as some details are short notice short duration jobs we may not have that luxury. If that is the case here are a few basic directions to go. If the patient is conscious, verbal, and in a clear but perhaps distressed state of mind start by obtaining a SAMPLE history.
S = Signs and Symptoms – what do you see, what can they or someone else tell you about their current condition
A = Allergies – do they have any they are aware of and do they take or have any medications related to them
M = Medications – do they take any medications, if so what for, and have they taken their medications today (be aware older clients in particular may have a long list of medications they are taking daily)
P – Past Illness – what is their past medical history; heart attack, stroke, asthma, diabetes, etc.
L = Last oral intake – when and what did they last eat or drink
E = Events leading up to the current condition – what was the patient doing just prior to what is happening now. Example: Were they playing tennis on a hot day and passed out.
–
If the patient is unconscious you will have to do a physical, assessment unless there is someone present that can explain what happened, even then you are still going to have to do a physical assessment. If that is the case here is some basic standard guidance. Unless there is an obvious arterial bleed, penetrating injury to the chest, or traumatic amputation (arterial bleeding, penetrating chest injuries which allow air to flow into the chest cavity and traumatic amputation need to be treated immediately) the basics are as follows, remember the mnemonic MARCH:
M – Massive Hemorrhage
A – Airway
R – Respiration
C – Circulation
H – Hypothermia Prevention
–
And of course, you have your ABC’s:
A – Airway – does the patient have a stable airway allowing oxygen to freely exchange
B – Breathing – is the patient breathing on their own at a rate that will sustain life (no less than six breaths per minute and no more than thirty breaths per minute for adults).
C – Circulation – is blood adequately circulating within the body. This can be checked by accessing the carotid, radial, and pedal pulses. (For small children and infants check the biracial pulse)
–
Treat the conditions you find and summon emergency medical help if the situation warrants in accordance with your SOP’s.
The amount and type of equipment you carry and utilize will depend on your training (I strongly recommend that anyone doing protective work minimally be CPR/ AED and basic first aid certified). Also the attire for your detail will influence what equipment you may be able to carry. Again I’m addressing details within CONUS. Most of the situations we deal with are usually not emergencies but headaches, stomachache, minor cuts and low impact trip and falls. Dehydration is a constant concern for both principals and members of the protective team. If you are the Detail Leader/ AIC, or team medic ensure that everyone is hydrating and getting some chow every few hours. One word on moving and injured person after a fall, vehicular crash, or other traumatic injury I recommend not moving them unless it is absolutely necessary due to safety concerns. Make them comfortable in place until EMS arrives and moves them for transport to a hospital. When limited to what I can carry on my person on a detail and keeping the appearance low profile my medical load out is as follows:
A small flat belt pouch or ankle pouch containing travel packets of Tylenol, Motrin, Imodium, Benadryl, alcohol wipes, a couple band aids, and a small bottle of hand sanitizer (I like the small ones that companies give out at trade shows. They are very small about .5 Oz. they are easy to carry and you can just refill them. Again whenever I can I like to know what the principal likes and can take, if not I’ll usually have a small assortment with one or two packets of each. You can be a hero if your principal has a headache or upset stomach and you can help him/her out without detouring to the nearest CVS, ADDED VALUE. Additionally I carry a small folding CPR pocket mask on my person, I prefer a hard shell but sometimes it is just too large for convince. My next line of medical equipment is my mini on my person trauma kit. This is kit is to bridge the gap kit until I can access a more comprehensive kit. I carry the following in a black ITS Tactical Slimline pouch: SWAT-T tourniquet, package of Quikclot sponge, pair of protective gloves, small roll of duct tape, and I tuck my Benchmade rescue hook in too (great for cutting seat-belts and clothing to expose injuries).
That is my basic on my person medical load out. If I’m working and have access to a vehicle or able to carry a backpack with me a more complete medical/trauma kit goes in there. The more space you have and the higher level of training you have the more options you have.” – Art Dorst, Consulting & Training Services
–
UPDATE 9-8-16
I was sitting at home last night watching John Wick again and I was thinking about the recent write up from AS Solutions authored by Eric Stewart. I’ve been an EMT for over twenty years and an American Red Cross Instructor for fifteen. Over the course of my professional medical provider career the organization I worked for provided my equipment. Since I’ve ventured out on my own that is no longer the case. Although I have not been designated as a team EMS provider my usual EMS Loadout is an IPAK and CPR face shield. After reading the article I thought to myself what if I got a call and was asked can you be at this location in four hours (not unusual for the companies I work for) and be the team emergency medical provider (Currently I work under the certification as an Emergency Medical Responder as opposed to my EMT certification for insurance and liability reasons). I realized that although I have a good bit of supplies it’s not organized nor did I have an effective and low profile means to carry it. I considered purchasing one of the STOMP packs mentioned in the article but that just isn’t doable right now (it is however on the to-buy list).
So I looked around my place and gathered up some assorted items that I felt could work. I started with a 5.11 molle panel and attached pouches to house my supplies. I used my CSM Gear EMT shear & Purell pouch, GORUCK utility pouch for my hard-shell CPR mask, a Condor EMS pouch for my Stethoscope, BP cuff, airways (oral/nasal), triangular bandages, roller gauze, and tape. On the flip side is a Blue Force Gear Trauma pouch with chest seals, Quikclot, Israeli bandages, and Tourniquets. Also on the back is a Blue Force Gear Boo Boo pouch containing Tylenol, Imodium, a chapstick, band aids, and other quick to grab items. There is an Endom Glove pouch and finally a Tactical tailor utility pouch with basic first aid items. This panel nests very nicely in my GORUCK GR1, I like this pack because it opens clam shell style allowing me quick access to the panel and other items I may need in an emergency. Yeah everything doesn’t match and there are a few items I’d like to pick up to increase my capabilities but all in all I’m pretty happy with it and feel I can rollout on short notice comfortable with my equipment. It doesn’t require a ton of money most of us have gear laying around innovate. We are at war, adapt. – Art Dorst, Consulting & Training Services

Equipment Sources: GORUCK, 5.11, CSM Gear, Condor, Blue Force Gear, Endom USA, Tactical Tailor
–
———————————————————
Joseph M. LaSorsa, CPP® is currently employed as a senior partner managing and conducting: Protective Operations Training Courses, Executive Protection & Bodyguard Services, Risk Management Consultations & Seminars, Workplace Violence Prevention Seminars & Intervention Services, Security Consultations & Seminars, Private Investigations and Technical Surveillance Counter-Measures with LaSorsa & Associates – an International Protection, Investigations & Consulting Firm.
https://www.linkedin.com/in/josephmlasorsa
